.svg)
Hope springs eternal. So does the phase 1/2 ReDiscover study, apparently.
Relay Therapeutics has kept zovegalisib's first clinical trial alive as a real-world optimization lab for the molecule. The study began with routine dose escalation evaluations, but has been adapted and expanded multiple times with data-informed decisions.
For example, triplets were originally intended to be optimized in the CDK inhibitor (CDKi) naïve population, but are now being optimized in the CDKi-experienced population. That strategic move could reduce the development timeline by roughly 12 months, which would make up for the delay caused by switching the recommended phase 3 dose (RP3D) right before starting the pivotal study.
The company made that decision before it had the clinical data to support it, instead showing confidence in its model-informed drug development (MIDD) approach.
Luckily for you, nervous investor, the supporting clinical data have arrived. The RP3D performed almost identically to the RP2D. Some metrics were a little worse and some metrics were a little better, but the overall data are consistent.
This serves as a great reminder of the value of the company's overall approach. Investors often focus on the drug discovery aspect of a technology platform, but that only finds you a molecule. You still have to go optimize the damned thing.
Relay Therapeutics does that by designing flexible clinical trials that can be right-sized on the fly with the latest data update. Maybe it wants to alter dosing, add a new CDK4 inhibitor to the program, or recruit a new population to explore a new idea quickly. The phase 1/2 ReDiscover study has been refined so many times it may end up supporting seven different pivotal studies.
I hope they wrote in pencil.
My point is that clinical trial optimization is also part of the technology platform. It's not just the fancy protein motion simulations that increase the probability of success. This is what MIDD and quantitative system pharmacology (QSP) look like in the real world.
In this case, the 400 mg dose of zovegalisib twice-daily with food appears remarkably similar to the 600 mg dose twice-daily on an empty stomach. By understanding that before designing a slate of pivotal programs, Relay Therapeutics increased the probability of success across at least three large commercial opportunities in CDKi-naïve breast cancer, CDKi-experienced breast cancer, and vascular anomalies.
How Do the RP3D Data Compare to RP2D Data?
From a statistical standpoint, the best investors can say is that the RP3D data are equivalent to the RP2D data. But that's no fun.
For clarity:
- The RP2D was 600 mg of zovegalisib twice-daily on an empty stomach (fasted)
- The RP3D is 400 mg of zovegalisib twice-daily with food (fed)
- Both were evaluated in combination with the estrogen-receptor degrader fulvestrant in patients with HR+/HER2- breast cancer who had received at least one prior line of treatment. That means the zovegalisib combo was at least the second-line (2L) of treatment each patient received.
- This specific indication is also referred to as the CDKi-experienced population because all patients had previously received a CDK4/6 inhibitor.
Keeping track of the data can be tricky. Investors have to weigh tolerability by looking at the incidence of side effects. Efficacy is reported on an overall basis and split between treatment lines, PI3K-alpha mutations, ESR1 mutations, and more.
Let's break it down starting with tolerability, which is measured in the overall patient population.
Tolerability profile of RP3D vs. RP2D
Tolerability profiles in the CDKi-experienced patient population are determined primarily by Grade 3 side effects, which were equivalent for the RP3D and RP2D.
Relay Therapeutics had hoped that the RP3D would reduce the incidence rate of upper gastrointestinal side effects like nausea, decreased appetite, and vomiting. That didn't happen. These side effects occurred at the same rate as the RP2D. Meanwhile, some side effects were actually more frequent when zovegalisib was taken with food.
Does this matter?
Treatments are often discussed in the context of tolerability, which takes into account the severity of side effects and the indication. For the CDKi-experienced breast cancer population, tolerability hinges on the rates of Grade 3 side effects. By that measure, the RP3D and the RP2D are equivalent.
Keep in mind these are relatively small cohorts of roughly 60 patients each. Every patient that experiences a side effect increases the incidence rate by 1.6% (1/60). Differences between these cohorts could be simply due to randomness and individual patients.
This is why larger studies are important. Individual patients in the pivotal ReDiscover-2 study will only increase the incidence rate by 0.4% (1/270), which will reduce noise and randomness.

The severity of side effects generally predicts discontinuations, but patients can discontinue treatment if they find less severe side effects difficult to manage. For example, the two discontinuations at the RP2D were from Grade 1 itch and Grade 1 nausea and loss of appetite.
There were four discontinuations at the RP3D, which represents a discontinuation rate of 6.7%. Investors want this to be as low as possible, but under 10% is solid for a heavily-treated patient population.
Importantly, the tolerability of the RP3D continues to compare favorably to the pivotal study comparator Truqap.

Overall patient characteristics of RP3D vs. RP2D
The overall patient populations were equivalent for the RP3D and RP2D cohorts. Several characteristics benefited responses in the RP3D cohort, while others made it more difficult to drive responses.
Tolerability profiles are primarily driven by dose levels, dose frequency, and the molecules used in combinations. Efficacy is driven by tolerability (the longer patients tolerate treatment the more likely they are to have a response) and the characteristics of the patient population.
The overall patient populations for the RP3D and RP2D cohorts were equivalent, but the differences were slightly more notable than for tolerability comparisons.
A few characteristics made the RP3D cohort more difficult to treat than the RP2D cohort. More patients had prediabetes (43% vs. 34%), a body mass index (BMI) above 30 or blood glucose levels above 5.7% (48% vs. 34%), or visceral tumors (72% vs. 61%). These characteristics typically reduce objective response rate (ORR), median progression-free survival (mPFS), and clinical benefit rate (CBR).
A few characteristics also made the RP3D cohort easier to treat. There were more 2L patients (60% vs. 55%) and patients with a kinase mutation (55% vs. 48%) than before, both of which would be expected to increase the overall ORR.

Astute investors might pick up on a few additional data points based on comparisons to the update from the San Antonio Breast Cancer Symposium (SABCS) in December 2025.
At last year's conference, Relay Therapeutics presented more granular RP2D data. Patients who had previously received fulvestrant have better responses to zovegalisib, as did patients with an ESR1 mutation. However, patients with an ESR1 mutation experienced disease progression sooner despite achieving deeper tumor reductions.
The RP3D cohort had fewer patients who had previously received fulvestrant (making it more difficult to drive responses), but also had more patients with an ESR1 mutation (making it easier to drive responses, but also reducing mPFS).
Efficacy of RP3D vs. RP2D, overall patient population
The overall population includes both 2L and 3L+ patients. Individuals receiving earlier lines of treatment typically have better responses.
The RP3D performed virtually identically to the RP2D in the overall population. However, the median follow-up occurred at 12.0 months for the RP3D data readout, much shorter than the 20.2 months for the prior dose. That creates the possibility for improving responses over time at the RP3D.
The mPFS, ORR, and CBR were equivalent in the overall population.
Management previously said it didn't expect a difference between kinase or helical mutations, which wasn't supported by previous data but might be true after all. Although the mPFS in kinase mutations dropped sharply at the RP3D (11.2 months vs. 18.4 months), a closer look at the RP2D data suggests they were driven by outliers.
This metric is measured using Kaplan-Meier curves. When half of patients stop responding, that point in time is used to calculate the median PFS. The RP2D had an unusually long plateau before reaching the median, which suggests the qualifying event just so happened to be dependent on super-responders. At the same time, the Kaplan-Meier curves for the RP3D suggest the overall mPFS might fall somewhere between 11 months and 14 months in a larger study.

Another important metric is whether or not circulating tumor DNA (ctDNA) for prominent cancer-driving mutations can be detected. The company has reported these metrics measured from the first day of the second treatment cycle (C2D1), which in this context is determined by fulvestrant administration. That means C2D1 occurs on Day 29.
The percentage of patients who experienced a reduction in ctDNA of PI3K mutations was equivalent between the RP3D and RP2D (93% vs. 97%). That includes 76% of patients who had no detectable PI3K mutations by C2D1 at the RP3D.
However, the RP3D doesn't appear as effective in reducing ctDNA for ESR1 mutations, which are associated with worse prognosis in HR+/HER2- breast cancer. There also appears to be a typo in the data communicated by the lead investigator of the study Dr. Andreas Varkaris. He states four patients didn't experience a reduction in ctDNA for ESR1 mutations, but the graphic clearly shows five patients failed to benefit on this metric. That means 76% (16/21) experienced a reduction, not the 81% (17/21) reported by him and Relay Therapeutics. Or the graphic is wrong. I'll be conservative just in case.
I can't offer a reason for the difference between the RP3D and RP2D. Although the current dose is lower, the distribution and blood concentration of zovegalisib is equivalent between doses. It may simply be due to the relatively small number of patients in these cohorts with an ESR1 mutation (21 for RP3D and 15 for RP2D). Such mutations occur in only 25% of the patient population that also have a PI3K-alpha mutation. Patients were enrolled in this specific study based on having a PI3K-alpha mutation, so ESR1 mutation status is more random for this study design.
Total discontinuations were more favorable for the RP3D than the RP2D (71% vs. 80%). This shouldn't be confused with discontinuations due to tolerability issues, which stood at 6.7% (4/60) and 3.1% (2/64), respectively. Rather, total discontinuations capture how many individuals stopped treatment for any reason, including tolerability issues, physician choice, no-showing follow-up appointments, or disease progression. Most patients discontinue treatment due to disease progression.
This also creates the possibility that RP3D responses will improve with time.
- One evaluable patient remains on treatment at the RP3D who hasn't experienced an objective response. If they respond, then the ORR could increase to 46% (16/35).
- Five patients remain on treatment who have already achieved an objective response. If they continue responding, then they will increase the overall mPFS beyond 11.1 months.
- Eleven (11) more patients remain on treatment but were not yet evaluable for efficacy at the time of the data cutoff. These patients are excluded from current ORR calculations (they're not in the denominator of 35 evaluable patients), which means their impact on efficacy is unknown.
Efficacy of RP3D, 2L vs. 3L patient populations
Patients who have received fewer lifetime treatments typically have better responses. That's because receiving treatment alters the genetic and molecular composition of tumors.
When dividing the overall patient population between 2L and 3L+ patients, the RP3D had equivalent efficacy to the RP2D.

How Do These Data Impact the CDKi-experienced Commercial Opportunity?
Relay Therapeutics is well-positioned to earn global regulatory approvals for zovegalisib in the CDKi-experienced breast cancer population.
The RP3D has a favorable tolerability profile compared to its active comparator and current market leader Truqap and appears to have a meaningful efficacy advantage. I would expect Truqap to deliver an mPFS above 5.5 months in the pivotal ReDiscover-2 study (higher than its own pivotal study) due to the enrollment criteria, but if zovegalisib can achieve an mPFS of at least 11 months then it should have a positive data readout.
Whereas every other PI3K pathway inhibitor has been evaluated in studies comparing to placebo, Relay Therapeutics is the first to use an active comparator – and the current market leader at that. Considering Truqap from AstraZeneca soared to full-year 2025 revenue of $728 million – and in only its second year on the market – the potential for zovegalisib to quickly steal market share is very tangible.

I hope investors understand the significance.
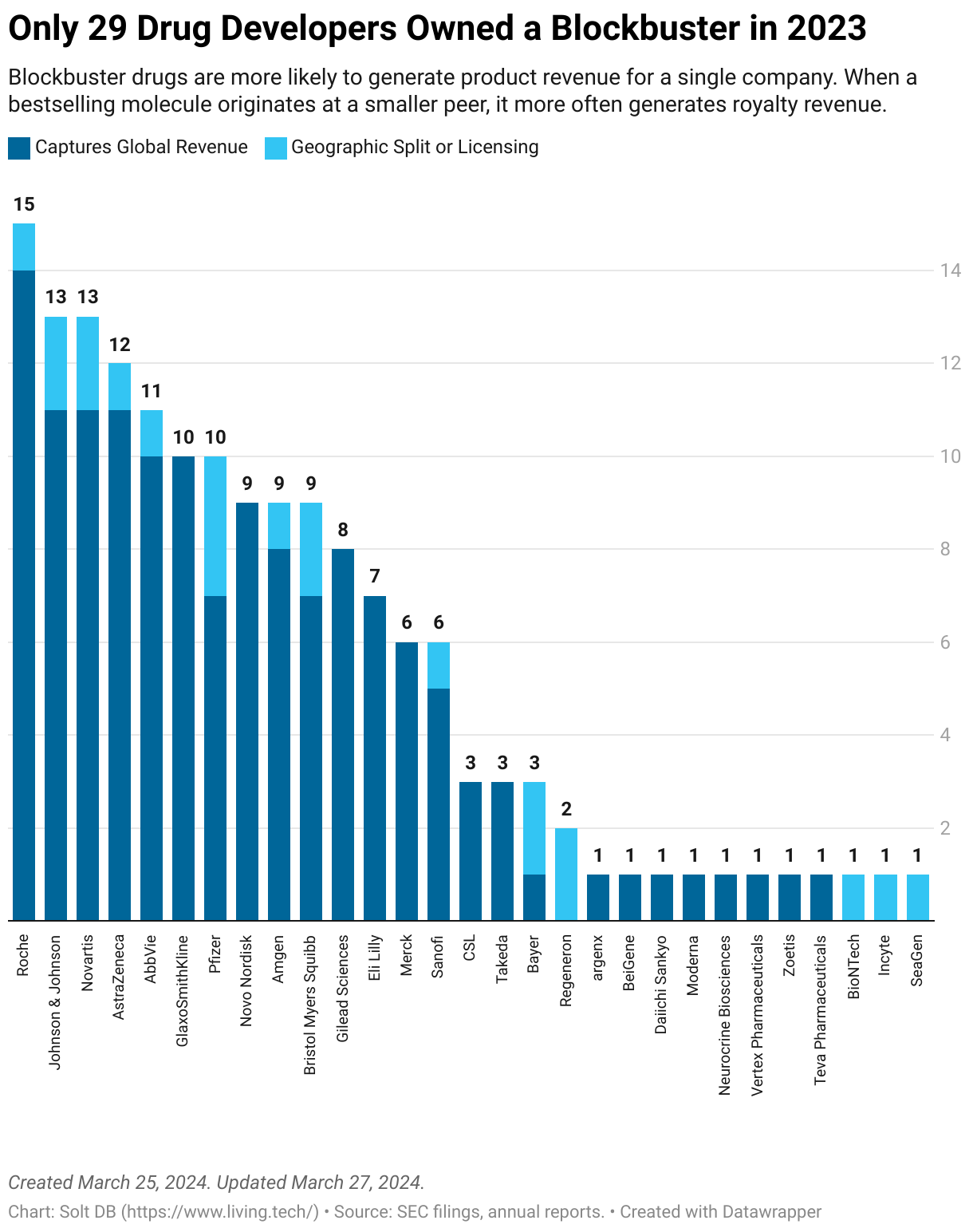
Sure, every drug developer talks about the blockbuster potential of their drug candidates. Every drug candidate is held up as "first-in-class" or "best-in-class" or has a gajillion dollar market opportunity. How many actually deliver though?
Very few.
Consider the handful of global companies that owned a drug product with at least $1 billion in annual revenue in 2023. Almost every company is valued in the tens of billions of dollars.
How Do These Data Impact Other Commercial Opportunities?
Although the RP3D of zovegalisib delivered no discernible advantages over the RP2D in the CDKi-experienced patient population, moving forward with the reduced dose has advantages for other commercial opportunities.
Tolerability
The bar for tolerability rises with the duration of treatment. Investors typically think of tolerability from the perspective of side effects, but reducing the daily pill burden from six at the RP2D to four at the RP3D also helps from a patient perspective.
- The CDKi-experienced patient population represents the lowest bar to clear for tolerability. That means less tolerable treatments can still capture market share.
- The CDKi-naïve patient population will likely receive zovegalisib triplets for twice the duration as their 2L peers (>24 months). That makes tolerability even more important. This is one reason Itovebi triplets are struggling to gain commercial traction, although that seems to be driven by CDK4/6 inhibitors.
- The vascular anomalies populations may receive zovegalisib monotherapy chronically, potentially for life and sometimes beginning in childhood. That makes tolerability critical to the commercial opportunity. In the dose escalation portion of the phase 1 ReInspire study, Relay Therapeutics is evaluating the RP3D from the pivotal ReDiscover-2 study as the highest dose level. It will benefit from not needing fulvestrant (or its associated side effects) in this population. Additionally, the goal would be to move all eligible patients to a long-term, lower-dose as a maintenance therapy.
Efficacy
Relay Therapeutics developed zovegalisib to capture the large, proven, and yet untapped market opportunity for PI3K-alpha inhibitors. The molecule appears to avoid Grade 3+ hyperglycemia – the showstopper side effect for the drug class – and common off-target side effects such as rash and mouth sores. That increases the potential to be used in combinations for CDKi-naïve breast cancer and as a chronic treatment for vascular anomalies.
- In the CDKi-experienced population (2L+), mPFS is the most important metric because it measures delaying disease progression in individuals who have already stopped responding to at least one prior treatment.
- In the CDKi-naïve population (1L, future triplets), overall survival (OS) is the most important metric because it measures the possibility of eliminating cancer. Although Relay Therapeutics doesn't have OS data available, CBR is a metric captured earlier in development that correlates to OS.
In the vascular anomalies population, efficacy will be measured differently than for cancer. An objective response in breast cancer is a reduction in tumor volume of at least 30%. In vascular anomalies, a tumor that shrinks by at least 20% is considered an objective response.
The time points for measuring and reporting efficacy are also different. Cancer generally involves mortality. A patient who first responds at Week 24 is just as good as one who responds at Week 2. In vascular anomalies, efficacy is strictly measured based on the duration of treatment and continued reductions in tumor volume over time.
The first preliminary data readout from the phase 1 ReInspire study will specifically share response rates at Week 12. The highest reported response rate at this checkpoint from the competitive landscape is just 16%. The highest response rate at any checkpoint is 33%. If zovegalisib has a leading tolerability profile and is the most selective molecule, then it should be able to deliver significantly higher efficacy.
If patients respond to zovegalisib with long-term use, then they may be able to transition to lower doses for maintenance treatment. It's an important part of the overall commercial opportunity, but investors won't have maintenance data in hand until the early 2030s.
News Flow & Modeling Insights
(No change.)
The current model makes the following assumptions:
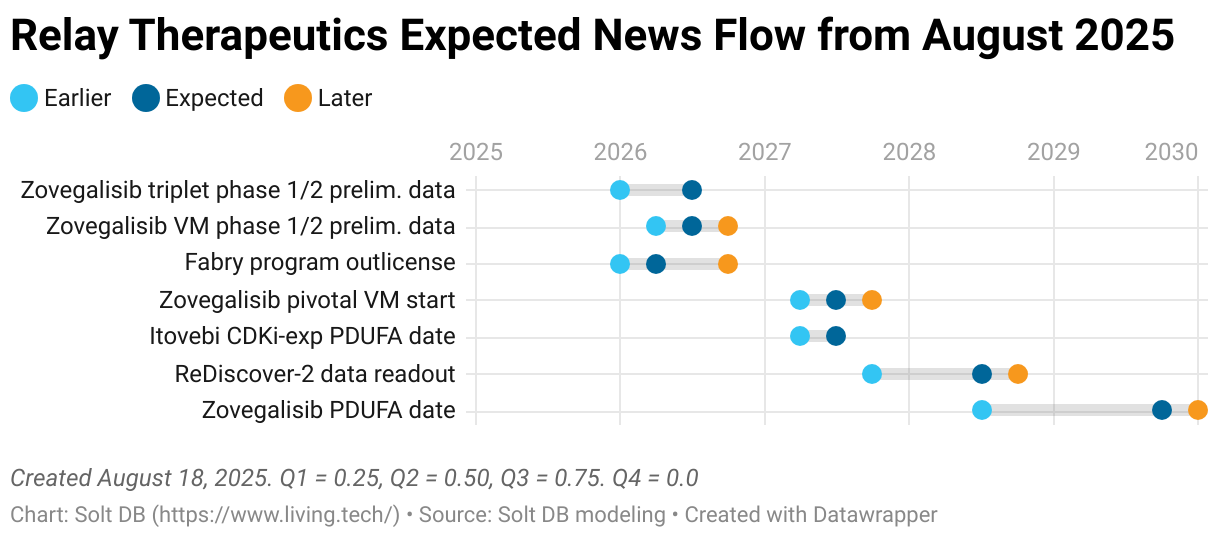
- The pivotal ReDiscover-2 study has a topline data readout in Q3 2028.
- Zovegalisib is submitted with a standard 10-month regulatory review. (It takes a few months from data readout to regulatory submission.)
- Zovegalisib launches in Q4 2029 with an approval in at least kinase mutations. A companion diagnostic required for this label claim is developed without delays.
- Zovegalisib generates full-year 2029 revenue of at least $45 million and full-year 2030 revenue of at least $600 million.
The expected news flow for Relay Therapeutics:
Margin of Safety & Conviction
(No change.)
Relay Therapeutics is considered a Future Compounder position with the following Conviction rating.
- 1 = High
- 2 = Above Average
- 3 = Average
- 4 = Below Average
The estimated fair valuation based on my current model is below:
- Market close March 18: $9.93 per share
- Modeled Fair Valuation: $17.68 per share
- Allocation Range: Up to 15%
Relay Therapeutics reported 178.725 million shares outstanding as of February 20, 2026. The modeled fair valuation above assumes 237.5 million shares outstanding, which is equivalent to full dilution expected through the launch of zovegalisib.
Further Reading
- March 2026 press release announcing RP3D data for zovegalisib
- March 2026 research note discussing full-year 2025 results and the outlook

.svg)
.svg)
.svg)


.svg)



.svg)
.svg)
.svg)